{kind=link}
This Article is a part of
Computer Vision Resource Center
Healthcare has always been a data-intensive profession. What has changed is the speed, volume, and complexity of that data — and the tools now available to make sense of it in real time.
Artificial intelligence in diagnostics is not a future concept being piloted in research labs. Right now, in 2026, it is embedded in radiology reading rooms, stroke triage workflows, cardiology monitoring systems, and pathology departments across thousands of hospitals globally. The FDA authorized a record 295 AI/ML-enabled medical devices in 2025 — a figure that would have been unimaginable a decade ago, when the annual total stood at six. The cumulative count reached 1,451 authorized devices by end of 2025, and that number is climbing faster than at any point in the technology’s history.
But authorization numbers only tell part of the story. The more important question — the one this guide addresses — is what these tools actually do in clinical settings, how they get from development to deployment, where they fall short, and what healthcare leaders, clinicians, and developers need to understand before making integration decisions in today’s environment.
Last year’s data tells us where AI diagnostics has been. This guide explains what those advances mean in practice and how healthcare leaders, clinicians, and developers can act on them today.
Table of Contents
Key Takeaways
- AI diagnostics has moved beyond pilot projects and is now integrated into radiology, cardiology, pathology, neurology, and primary care workflows.
- Clinical validation, interoperability, and governance are becoming more important than raw AI accuracy when selecting diagnostic platforms.
- The FDA’s Predetermined Change Control Plan (PCCP) framework allows approved AI systems to evolve safely after deployment.
- Hospitals should evaluate AI diagnostic vendors based on explainability, workflow integration, transparency, cybersecurity, and long-term monitoring—not marketing claims.
- The future of AI diagnostics lies in multimodal intelligence, combining imaging, laboratory data, genomics, wearable devices, and electronic health records.

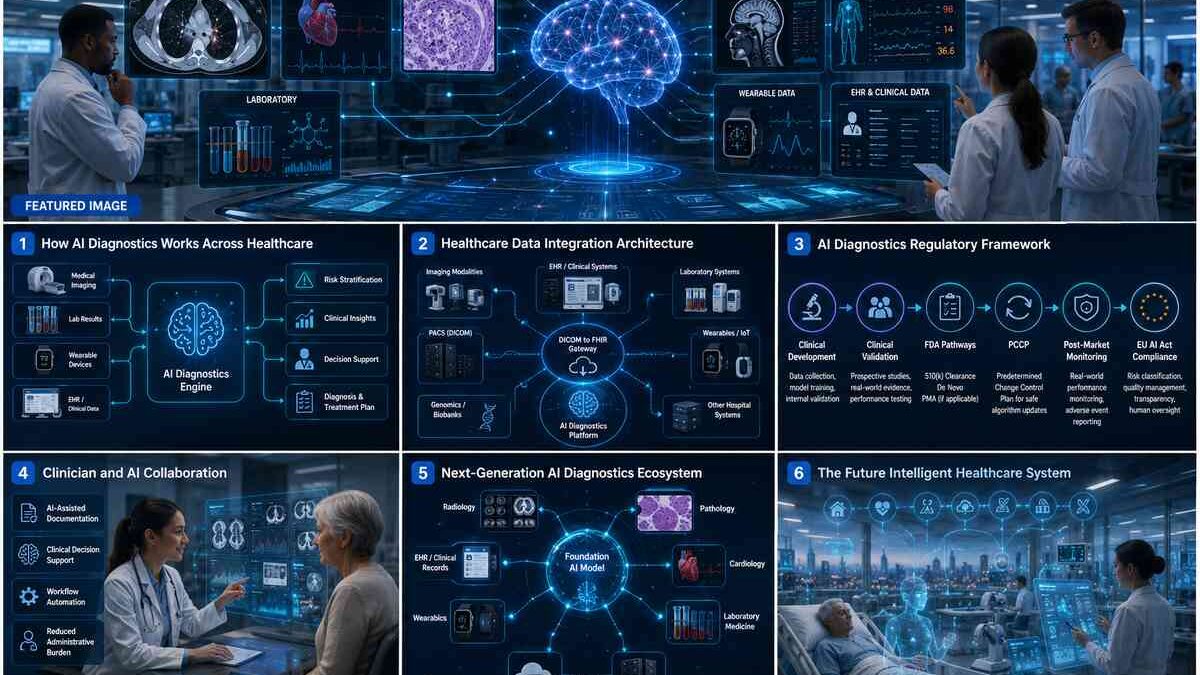
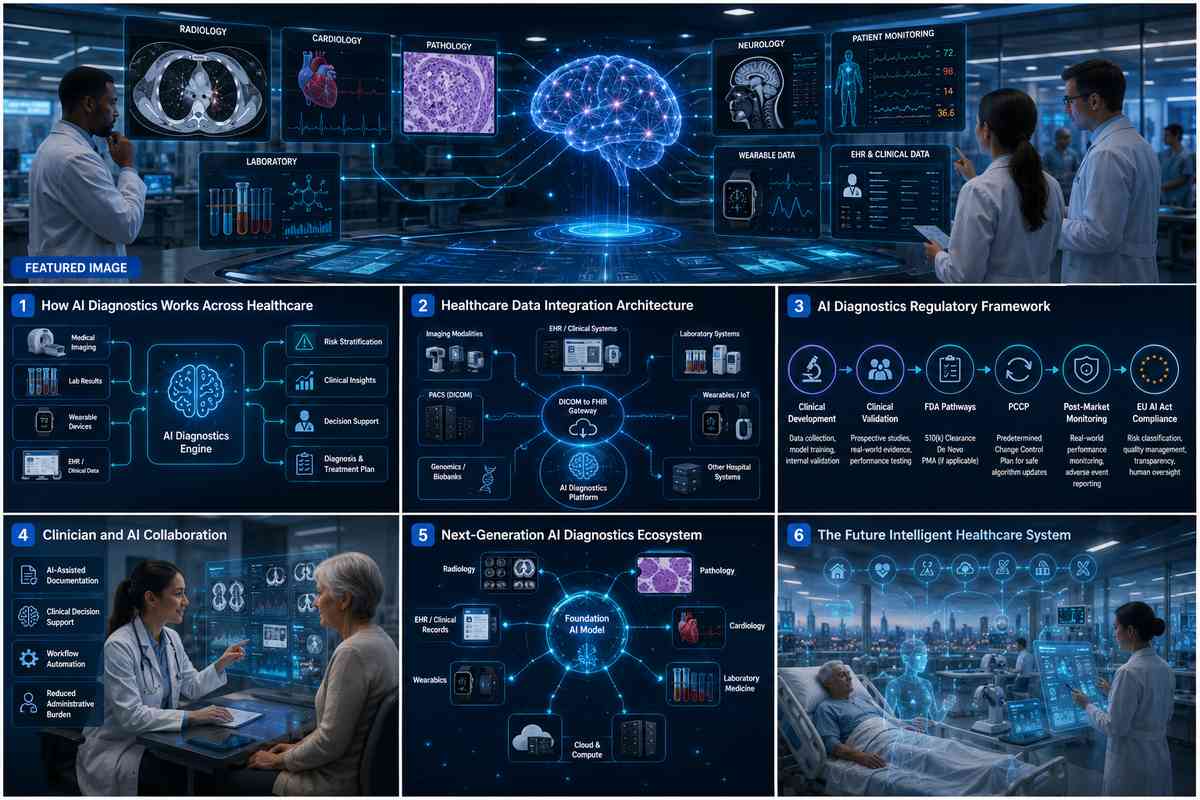
The Diagnostic Intelligence Layer: How AI Is Rewiring the Front Door of Care
For most of modern medicine’s history, diagnostics operated as a series of discrete, reactive events. A patient presented with symptoms. A test was ordered. A result came back. A clinician interpreted it and decided what to do next. The process was inherently episodic — a snapshot, not a continuous picture.
Artificial Intelligence is beginning to slowly upset that model, and the process is structural and rather than moderate.
Over the last 12–18 months, in many of the largest health systems in the country, what we call the Diagnostic Intelligence Layer has developed, a global infrastructure fusing genomic profiles, imaging results, biosignals from wearables, and EHRs into a continuous, fluid loop. Rather than stratified measurements, patients now present with risk gradients and whole-life pathways; rather than arbitrary assessment, AI presents anesthesia-monitor alarms befire catastrophe.
And how does this look today? The patient who has a prior diagnosis of hypertension, is at home in a student-tended setting with a over-the-counter cardiac monitor implanted on him. The machine detects an abnormal rhythm at 2 am, and runs the input through a clinical AI model facilitated by an EHR noting that his father has atrial fibrillation and his inflammatory markers are elevated today and delivers a risk-stratified alert to his physician before he even makes a timed appointment.2 Apple‘s AFib clinical tracking history monitor has already brought high fidelity cardiac diagnostics into the world of consumer wearables, and these clinical effects are reverberating across cardiology departments.
Routine biomarkers, GLP-1 monitoring data, and continuous glucose readings are no longer standalone test results. They are longitudinal intelligence streams — and the health systems that have built the infrastructure to interpret them continuously are operating with a fundamentally different clinical model than those still managing episodic diagnostics.
The Technical Bridge That Makes This Possible
The architecture enabling this shift depends on one critical integration layer: DICOM-to-FHIR gateways.
Here is the problem these gateways solve. Imaging data — X-rays, CT scans, MRIs — lives in PACS systems in DICOM format. Clinical history — smoking status, medication records, family genetics, lab results — lives in EHR systems in entirely different formats. Until very recently, these two types of data never ‘talk’ to each other in a meaningful way. An AI model and ‘looking at’ a Chest CT could not have programmatically ‘known’ that the patient had been a smoker for 30 years or that her father had lung cancer.
DICOM-to-FHIR integration converts image metadata into standard FHIR resources, which create a direct connection between pixel-level findings and the patient‘s longitudinal record. The result is context-aware diagnostics — AI models that weigh imaging against clinical history to produce genuinely actionable risk assessments rather than isolated pattern detections.
This architectural shift matters because accuracy without context is a limited clinical tool. A chest nodule detected in isolation means one thing. That same nodule in a 58-year-old former smoker with elevated CEA levels means something considerably more urgent. The health systems investing in this integration infrastructure today are building the diagnostic foundation that will define competitive clinical positioning for the next decade.

Comparison of Major AI Diagnostic Technologies
| Technology | Primary Use | Strengths | Current Limitations |
| Machine Learning | Predictive analytics | Fast structured data analysis | Limited contextual understanding |
| Deep Learning | Medical image interpretation | Excellent pattern recognition | Requires large labeled datasets |
| Foundation Models | Multi-specialty diagnostics | Highly adaptable across tasks | Still requires extensive clinical validation |
| Generative AI | Clinical documentation and reporting | Reduces administrative burden | Requires strong human oversight |
From Triage to Automated Detection: Where AI Is Delivering in 2026
The clinical applications of AI diagnostics are not evenly distributed. Some specialties have moved faster, built larger evidence bases, and attracted more investment than others. Understanding where the technology is genuinely delivering — and where it is still maturing — is essential for any implementation decision being made right now.
Radiology: The Established Intelligence Layer
In 2025, radiology made up 71.5% of all FDA AI/ML clearances and is still by far the most prevalent clinical specialty for diagnostic AI as we look ahead to 2026. This is not by chance. Radiology was among the first medical specialties to fully digitize, which means it accumulated the large, structured datasets that deep learning models require. Product Code QIH — Radiological Computer-Aided Detection — accounted for 75 clearances in 2025 alone, representing the single largest regulatory cluster in the entire AI medical device landscape.
Real-world performance data from last year’s deployments is increasingly compelling and shaping purchasing decisions in 2026. GE HealthCare’s Air Recon DL platform uses deep learning reconstruction to deliver 50% faster MRI acquisition times while simultaneously improving image quality. Over 34 million patients have undergone scans processed by this system — a deployment scale that makes it one of the most clinically tested AI diagnostic tools in existence.
In breast imaging, AI-assisted reading tools demonstrated 33% reductions in image interpretation time without compromising diagnostic accuracy in 2025 deployments. For departments managing radiologist shortages and growing imaging volumes simultaneously, that throughput improvement is not a marginal gain — it is an operational lifeline.
The clinical impact extends beyond speed. AI models trained on mammography data have shown sensitivity rates for early-stage breast cancer detection that rival experienced radiologists in controlled studies. The critical caveat — one that responsible procurement teams must hold onto — is that real-world generalizability across diverse patient populations remains an active area of research and scrutiny. Controlled study performance and real-world deployment performance are not the same number.
Cardiovascular and Neurology: High-Stakes, Time-Critical Applications
Cardiovascular AI represented 8.8% of 2025 clearances, and most of these were in the domain of ECG signal analysis and arrhythmia detection. There is a clear clinical justification for these applications as cardiac events are time critical, ECG signals are block-structured and standardized, and the cost of false negatives is catastrophically high. In 2026 these tools are transitioning from pilot deployments towards integrated standard-of-care at advanced health systems.
Neurology represents 4.7% of clearances, with the most rigorously documented applications centered on large vessel occlusion detection and stroke triage. The data from the 2025 International Stroke Conference on the Viz.ai platform continues to serve as the benchmark evidence case for AI diagnostic ROI:
44% reduction in Door-In-Door-Out (DIDO) transfer times — nearly 90 fewer minutes in interfacility coordination
31-minute acceleration in treatment initiation — directly aligned with the clinical principle that in stroke care, time is brain tissue
84% faster care-team notification — dropping from 45 minutes to 7 minutes post-scan
For hospital C-suites evaluating AI investment in 2026, the economic translation of this performance is equally important. For Primary Stroke Centers, AI-powered coordination translates to a projected $36.7 million reimbursement shift by enabling regional centers to appropriately manage patients who would previously have required futile high-acuity transfers. That is not a soft benefit — it is a measurable financial reconfiguration enabled by a single well-implemented AI tool.
Digital Pathology and Emerging Specialties
Digital pathology is earlier in its AI integration curve but represents a high-value development area being actively watched in 2026. Tumor classification is cognitively demanding work — pathologists must visually assess tissue samples under time pressure, often with significant interobserver variability. AI tools in this space are specifically targeting cognitive load reduction rather than replacement, helping pathologists focus analytical attention on genuinely ambiguous cases while automating classification of clear-cut findings.
Gastroenterology and urology together account for 2.4% of clearances, with polyp detection during colonoscopy representing the most clinically validated application in this category. Pulmonary care AI is making meaningful inroads in radiation treatment planning, where models demonstrated measurable reductions in radiation contouring variability in 2025 — a task that has historically shown high inconsistency between treatment centers and between individual practitioners.
Navigating the FDA Pathway: What the 2025 Data Tells Us About 2026 Decisions
Comprehending the pathways through which these AI diagnostic tools will be adopted into clinical practice in 2026 is essential knowledge for any health organization leader making procurement and research and development decisions in 2026. It is foundational due diligence.
The 510(k) Dominance — and Its Limitations
In 2025, 97% of AI/ML medical device clearances went through the 510(k) route, where companies prove “substantial equivalence” to an already owned, legal predicate device, in lieu of doing a standalone randomized controlled trial. The median time to clearance was 142 days, with average time at 150 days.
The strategic truth of this spatio-temporal concentration is worth an attentive consideration, especially for procurement teams that take tomorrow’s choice. The 510(k) pathway is faster, less expensive, and less evidentiary than the De Novo or PMA pathways — and for software devices that genuinely resemble validated predecessors, it is entirely appropriate. But the data reveals a transparency deficit that healthcare buyers in 2026 cannot afford to overlook:
Fewer than 2% of cleared AI/ML devices are supported by randomized controlled trial evidence
Fewer than 1% of FDA decision summaries report actual patient health outcomes — they report analytical performance metrics like sensitivity and specificity instead
This is not an indictment of the devices themselves. Many perform well in practice. But it functions as a mandatory due diligence checklist for hospital procurement teams in 2026. Before signing any vendor contract, the following questions require documented answers:
- Has this tool been tested on a patient population similarincharacteristicsto yours?
- Has it been tested on an EHR as comparable to yours as possible?
- What are the post-deployment performance monitoring commitments?
- What happens when performance degrades in your specific patient population?
The FDA’s De Novo pathway — used by a small fraction of AI devices — offers a higher evidentiary standard and is appropriate for genuinely novel tools without clear predicates. The IDx-DR autonomous diabetic retinopathy screening tool, which can provide a screening diagnosis without specialist intervention, received clearance through this route. For procurement teams specifically evaluating autonomous AI tools, De Novo clearance carries meaningfully more evidentiary weight than 510(k) and should be weighted accordingly in vendor comparisons.
The PCCP Framework: The Most Important Regulatory Development You Need to Understand in 2026
The Predetermined Change Control Plan (PCCP), finalized by the FDA in late 2024 and now actively deployed across the 2025 clearance cohort, is the most operationally significant regulatory development shaping AI diagnostics right now.
The PCCP represents a fundamental philosophical shift in how the FDA thinks about software regulation. Traditional medical device approval assumed a relatively static product — you submit, you get cleared, the device is what it is. Software does not work this way. Algorithms improve. Training data expands. Model architectures evolve. Under the previous framework, every meaningful algorithm update potentially required a new 510(k) submission — a process averaging 142 days each time.
PCCPs solve this problem by allowing manufacturers to pre-specify future modifications at the time of initial clearance. If the FDA authorizes the PCCP alongside the device, subsequent algorithm updates that fall within the pre-approved scope can be deployed post-market without new submissions — provided they follow the pre-validated testing protocols.
In 2025, nearly 10% of all AI/ML clearances included a PCCP and that number will likely increase dramatically throughout 2026 with companies adopting the framework for its strategic benefits. For health systems evaluating vendors today, a PCCP-equipped device signals both regulatory sophistication and a commitment to ongoing improvement — both of which matter for a tool your institution will depend on across multiple product generations.
The five governing principles of a valid PCCP that procurement teams should verify:
- Focused and Specific — modifications must be clearly defined, not open-ended promises of future improvement
- Protocol-Based — validation procedures must be pre-specified and reproducible, not discretionary
- Impact Assessment — rigorous evaluation of how changes affect safety and performance is mandatory
- Transparency — users must be clearly informed when updates occur and precisely what changed
- Ongoing Monitoring — continuous post-market performance tracking is a condition of the framework, not an optional add-on
The EU AI Act: The Compliance Crisis Arriving This Year
For any healthcare organization with international operations, 2026 is not the year to be monitoring the EU AI Act from a distance. The compliance deadlines are here.
The EU AI Act, effective August 2024, classified medical AI as “High-Risk” under Article 6(1) and Annex I. The practical implications are significant and immediate. EU market access for AI diagnostic tools requires substantially more rigorous evidence packages than the US 510(k) pathway demands — closer in evidentiary standard to what the FDA’s De Novo pathway requires than the 510(k) most cleared devices relied on.
The critical compliance deadlines are August 2026 and August 2027. Manufacturers who built their global commercial strategy around US 510(k) clearance alone are now facing a bifurcated compliance reality. The evidence packages required for EU High-Risk AI classification take substantial time to assemble — organizations that have not already begun this process are operating with shrinking runway.
For MedTech developers reading this guide in 2026: the time to have started EU AI Act compliance planning was 2024. The time to accelerate it aggressively is right now.

Beyond Accuracy: Solving the Black Box Problem in 2026
Accuracy metrics are necessary but not sufficient for clinical adoption. A radiologist will not systematically trust — or act on — a recommendation they cannot understand, audit, or explain to a patient. This is not technophobia. It is professional responsibility and, increasingly, legal exposure.
The “black box” problem refers to the opacity of deep learning models: they produce outputs without providing comprehensible explanations of how they reached them. A model that flags a pulmonary nodule as high-risk without indicating which imaging features drove that classification is not a complete clinical tool — it is an alert system that generates outputs without accountability.
Explainable AI (XAI) addresses this through several technical approaches that health systems should now be requiring from vendors as standard deliverables:
- Saliency mapping — visual overlays that highlight which regions of an image most influenced the model’s output, allowing radiologists to verify that the model is attending to clinically relevant features rather than imaging artifacts
- Feature attribution — quantifying which input variables contributed most to a prediction, enabling clinicians to understand the relative weight of imaging findings versus clinical history in AI-generated risk scores
- Confidence scoring — providing probabilistic ranges rather than binary outputs, allowing clinicians to calibrate their reliance on AI recommendations based on the model’s expressed certainty
The HTI-1 Rule: Your Legal Framework for AI Accountability
The ONC’s HTI-1 Final Rule has moved from regulatory announcement to active compliance requirement in 2026. It mandates that developers of “Predictive Decision Support Interventions” disclose 31 source attributes, covering:
- Training data origins and demographic composition
- External validation results in populations different from the training set
- Performance metrics stratified by race, sex, age, and comorbidity burden
- Fairness evaluation methodologies and outcomes
- Audit trail capabilities for individual predictions
This rule reaches approximately 96% of US hospitals through certified health IT systems. In practical terms, it means that AI diagnostic tools deployed in the vast majority of American hospitals are now subject to specific transparency standards — and vendors who cannot demonstrate compliance with these 31 attributes should not be in your procurement pipeline.
The Moral Crumple Zone: Why This Is Now a Liability Conversation
The concept of “moral crumple zones” has moved from academic ethics papers into hospital risk management meetings in 2026, and for good reason.
In the current legal landscape, when an AI tool produces an erroneous recommendation that contributes to patient harm, professional and legal liability does not distribute itself across the algorithm, its developer, and the deploying institution in any clearly defined way. In practice, it tends to fall disproportionately on the clinician who acted on the recommendation — the human in the chain who becomes the crumple zone absorbing the impact of the system’s failure.
For hospital risk management teams and procurement officers, this reality translates into concrete vendor accountability requirements. Before deploying any AI diagnostic tool in 2026, health systems should demand documented evidence of:
- Demographic representation in training datasets
- Subgroup performance metrics across diverse patient populations
- Clear institutional protocols for situations where AI output conflicts with clinical judgment
- Defined escalation pathways and accountability structures for AI-influenced adverse events
- Vendor liability positions for documented AI-related harm
Algorithmic transparency is not a regulatory checkbox. In 2026, it is a clinical governance prerequisite and an active liability management requirement.
Human-Centered AI: Addressing Burnout and the Adoption Reality
Clinician adoption is the last mile of AI implementation, and it is frequently where technically sound tools fail commercially and operationally. Understanding why requires acknowledging a reality that vendor marketing rarely addresses: the healthcare workforce is already operating at its cognitive and emotional limits.
Physician burnout prevalence reached 54.9% in recent survey data. Administrative burden — documentation, prior authorizations, routine communications — consumes an estimated two hours of clinician time for every one hour of direct patient care. Into this environment, poorly designed AI tools do not help. They add another system to learn, another alert to manage, another source of cognitive friction in an already overloaded workday.
The AI applications demonstrating the strongest adoption outcomes in 2025 and carrying that momentum into 2026 are those designed around workflow subtraction rather than workflow addition — tools that remove tasks from clinicians’ plates rather than adding new ones.

The Documentation Revolution
Generative AI clinical documentation systems represent one of the most impactful and rapidly scaling AI applications in healthcare right now. These tools — commonly called AI scribes — listen to clinical encounters and generate structured clinical notes, eliminating the post-visit documentation burden that clinicians have consistently identified as among the most demoralizing aspects of modern medical practice.
The outcome data from 2025 deployments is striking. AI digital scribes save clinicians an average of 1.5 hours of documentation time per week. In a six-month longitudinal study, implementing AI scribes was associated with a 21.6% reduction in burnout prevalence, dropping the measured rate from 54.9% to 33.3%.
These are not marginal improvements in a workforce crisis. They are meaningful, measurable shifts in the sustainability of clinical practice — and they represent the kind of tangible ROI that department heads and hospital administrators can bring to budget conversations with confidence.
The Alert Fatigue Problem
Alert fatigue deserves particular attention from implementation teams in 2026. Every unnecessary notification a clinician receives trains them to dismiss the next one. AI systems that generate high volumes of low-confidence alerts — or that flag findings the clinician would have identified independently — are actively degrading their own clinical utility and eroding trust in AI tools broadly.
Effective implementation requires calibrating alert thresholds to institutional workflows and establishing feedback loops that allow clinicians to report false positives and refine model behavior over time. This is not a one-time configuration task. It is an ongoing governance responsibility that requires dedicated clinical informatics support and a structured process for iterative model refinement based on real-world performance data.
In radiology specifically, AI-assisted reading workflows that pre-screen studies and flag normal cases — allowing radiologists to focus attention on flagged and complex findings — demonstrated measurable cognitive load reductions in 2025. For departments managing radiologist shortages alongside growing imaging volumes, this workflow redesign is becoming operationally essential rather than optional.
The Multimodal Present: Foundation Models, Generative AI, and the Ecosystem Taking Shape Now
The architecture of AI diagnostics has shifted meaningfully over the past 12 months. What was theoretical in 2024 is deployed or in active development in 2026.
The Foundation Model Reality
In February 2025, the FDA cleared Aidoc’s CARE1™ — the first foundation model to receive regulatory authorization for clinical use. Twelve months later, this milestone has moved from news event to active reference point for how the industry thinks about next-generation AI architecture.
- Traditional AI medical devices are narrow models: trained to perform a single specific task — detecting one fracture type, flagging one lesion category, analyzing one biomarker. Foundation models are architecturally different. They are large-scale models trained on diverse data types that can be adapted to multiple clinical tasks without being rebuilt from scratch for each application.
- The commercial promise is real: foundation models can meaningfully compress the time required to develop new clinical AI applications, since adaptation rather than reconstruction is the development pathway. However, a critical distinction must be maintained clearly in 2026 as vendor marketing around foundation models intensifies.
Algorithm development timelines and clinical validation timelines are not the same thing. A foundation model can be adapted to a new diagnostic task in weeks. Validating that adaptation for safety and performance across diverse patient populations still requires rigorous clinical study — and that timeline has not compressed at the same rate as the development cycle. Healthcare leaders evaluating foundation model-based tools must probe vendor claims about deployment speed carefully, ensuring that development speed has not come at the expense of validation depth.

The cumulative AI/ML leadership landscape as of end-2025 reflects both the foundation model shift and the continued dominance of established players:
| Rank | Manufacturer | Cumulative AI Device Clearances |
| 1 | GE HealthCare | 120 |
| 2 | Siemens Healthineers | 89 |
| 3 | Philips | 50 |
| 4 | Canon | 45 |
| 5 | Shanghai United Imaging | 38 |
While these established players dominate cumulative counts, 183 manufacturers achieved single clearances in 2025 — evidence of a vibrant startup ecosystem operating alongside the titans. Companies like Aidoc and Viz.ai represent a category of hyper-specialized innovators whose clinical focus and workflow integration depth frequently exceed what larger hardware-centric companies deliver in specific clinical domains.
Leading AI Diagnostics Companies in 2026
| Company | Primary Focus | Representative Solutions |
| GE HealthCare | Radiology AI | AIR Recon DL, Edison Platform |
| Siemens Healthineers | Medical imaging AI | AI-Rad Companion |
| Philips | Clinical workflow AI | Diagnostic imaging solutions |
| Aidoc | Clinical AI platform | Foundation models, radiology triage |
| Viz.ai | Stroke and cardiovascular AI | Stroke workflow automation |
The Infrastructure Layer: Nvidia, Wearables, and the Convergence
Infrastructure partnerships are actively reshaping the competitive landscape in ways that affect every health system making AI investments in 2026. Nvidia has become the hardware-accelerated processing layer beneath much of the industry’s AI capability, with strategic partnerships involving Medtronic and Johnson & Johnson providing the computational infrastructure that medical AI at clinical scale requires. Inference speed and model scalability depend directly on this hardware layer — a fact that matters when evaluating vendor scalability claims.
Simultaneously, the boundary between consumer health technology and clinical diagnostics is becoming increasingly permeable in ways that require health systems to update how they think about their diagnostic infrastructure. Apple’s AFib detection in consumer wearables is the clearest current example, but the broader trajectory toward clinical-grade continuous monitoring delivered through consumer devices is accelerating. For some patient populations, wearable biosignal data is becoming the primary longitudinal data stream informing clinical decision-making — not a supplement to episodic encounters.
Generative AI in Patient-Facing Roles: Promise With Appropriate Caution
The emergence of generative AI in direct patient interaction — tools like the RecovryAI surgical recovery chatbot — represents one of the more complex developments to evaluate in 2026. These tools are creating new touchpoints between health systems and patients in post-acute and recovery phases, with genuine potential for improving adherence monitoring and early complication detection.
The clinical evidence base for these applications is thinner than for imaging AI, and the governance questions around appropriate scope of interaction, liability for AI-generated patient guidance, and integration with clinical oversight workflows are still being actively worked out. Health systems deploying patient-facing generative AI in 2026 should ensure that clear escalation protocols to human clinicians are built into the product architecture — not bolted on as an afterthought.
Reimbursement in 2026: The Question Every Administrator Is Actually Asking
No analysis of AI diagnostics is complete without addressing the financial infrastructure question that governs real-world adoption decisions: are these tools reimbursable, and through what mechanism?
The honest answer in 2026 is that reimbursement for AI diagnostic tools has matured somewhat from its nascent state but remains a genuine complexity that no responsible analysis should minimize.
CMS has established Category III CPT codes for some AI-assisted diagnostic functions — temporary codes that track utilization and build the evidence base for eventual Category I permanent reimbursement status. A targeted set of AI tools, primarily in radiology and cardiac imaging, have achieved specific reimbursement recognition. The AMA CPT Editorial Panel has been actively reviewing code applications as the evidence base from 2025 deployments accumulates, and 2026 is expected to see continued incremental expansion of recognized codes.
Some health systems are increasingly pursuing value-based contract models with AI vendors, where payment is tied to demonstrated outcomes — reduced length of stay, avoided transfers, lower readmission rates — rather than fee-for-service billing. The Viz.ai stroke coordination data, with its $36.7 million projected reimbursement impact for regional stroke centers, illustrates precisely why this model is gaining traction: the economics of keeping appropriate patients in regional facilities rather than executing futile high-acuity transfers are compelling enough to fund AI investment even in the absence of direct CPT reimbursement.
For hospital CFOs building the business case for AI diagnostic investment in 2026, the reimbursement analysis needs to incorporate three distinct value categories:
- Direct billing — CPT codes where applicable and currently recognized
- Indirect revenue protection — avoided penalties, reduced readmissions, improved CMS quality metrics that affect value-based contract performance
- Operational savings — reduced labor costs through workflow automation, decreased overtime from faster throughput, avoided capital expenditure through efficiency gains
The full economic case for most AI diagnostic tools requires all three categories to make the investment math work convincingly. Single-category analyses — particularly those relying solely on direct CPT billing — will routinely understate or overstate ROI depending on which category they select.
The Future of AI Diagnostics Beyond 2026
Over the next several years, AI diagnostics is expected to evolve from individual decision-support applications into continuously learning clinical intelligence platforms. Rather than analyzing isolated imaging studies or laboratory reports, future systems will integrate multimodal data—including genomics, wearable biosensors, pathology slides, medication histories, and electronic health records—to generate more personalized diagnostic insights.
Healthcare organizations are also likely to adopt autonomous workflow orchestration, where AI prioritizes cases, monitors patient risk continuously, recommends follow-up actions, and assists multidisciplinary care teams. As regulatory frameworks mature and interoperability standards improve, AI diagnostics will increasingly become foundational clinical infrastructure instead of standalone software.
What Healthcare Leaders Need to Do Right Now
The 2025 FDA data has confirmed what many suspected: the experimental phase of AI diagnostics is over. What 2026 demands is implementation discipline — the ability to separate tools with genuine clinical and economic value from those riding the wave of category enthusiasm without the outcomes data to justify it.
Several priorities demand immediate attention:
Demand validation transparency as a procurement standard. Before any AI diagnostic procurement decision in 2026, require vendors to provide demographic composition of training data, external validation results in populations comparable to yours, and performance metrics stratified by relevant subgroups. The HTI-1 Rule’s 31 source attributes provide the accountability framework — use it as a vendor selection filter, not a post-contract compliance exercise.
Assess PCCP status in every competitive evaluation. When comparing vendors, ask specifically whether their cleared device includes an FDA-authorized PCCP. A PCCP-equipped device signals regulatory sophistication and a commitment to continuous improvement — qualities that matter significantly for tools your institution will depend on across multiple product generations as the clinical AI landscape continues evolving.
Build interoperability infrastructure before deploying AI tools. AI diagnostic tools consistently underperform when operating in data silos. Prioritize vendors whose integration architectures support DICOM-to-FHIR connectivity and demonstrate genuine EHR compatibility with your specific system environment. The tools and the data infrastructure need to be designed together, not retrofitted.
Establish governance frameworks before go-live, not after. Implement clear institutional policies covering clinician accountability for AI-influenced decisions, alert threshold calibration processes, feedback loop mechanisms for ongoing model refinement, and defined escalation protocols for situations where AI output conflicts with clinical judgment. Governance retrofitted after deployment problems emerge is governance that arrives too late.
Act on EU AI Act compliance immediately if it applies to you. If your organization has international operations or anticipates them, the August 2026 compliance deadline for EU High-Risk AI classification is not a future planning item — it is a current operational urgency. The evidence packages required take time to assemble. Organizations that have not already begun this process need to escalate it now.
Frequently Asked Questions
Q1: What is AI diagnostics?
A: AI diagnostics refers to the use of artificial intelligence to assist healthcare professionals in detecting diseases, interpreting medical data, prioritizing urgent cases, and supporting clinical decision-making.
Q2: Can AI replace doctors?
A: No. Current AI diagnostic systems are designed to augment clinicians by improving speed and accuracy, but final diagnosis and treatment decisions remain the responsibility of qualified healthcare professionals.
Q3: How accurate are AI diagnostic systems?
A: Accuracy varies depending on the clinical application, training data, and validation studies. Many FDA-cleared AI systems demonstrate excellent analytical performance, but real-world effectiveness depends on workflow integration and patient diversity.
Q4: What is a Predetermined Change Control Plan (PCCP)?
A: A PCCP allows manufacturers to update AI algorithms under an FDA-authorized framework without submitting a completely new regulatory application for every approved modification.
Q5: Why is explainable AI important in diagnostics?
A: Explainable AI improves clinician trust by showing how algorithms reached a prediction, making it easier to validate recommendations, identify potential bias, and support regulatory compliance.

The Bottom Line
AI diagnostics in 2026 is not a single technology. It is a rapidly evolving infrastructure layer touching every dimension of how clinical information is generated, interpreted, shared, and acted upon. The tools delivering genuine value share identifiable characteristics: they integrate contextually rather than operating in data silos, they are designed around clinical workflow realities rather than technical capabilities alone, they are transparent enough to earn and maintain clinician trust over time, and they are governed by institutional frameworks that assign accountability clearly before something goes wrong.
The market is large. The investment is significant. The clinical promise is real and increasingly documented. But the evidence base is thinner than adoption rates suggest, the regulatory landscape is bifurcating in ways that create genuine compliance risk for global operators, and the workforce and interoperability barriers to scale remain substantial challenges that enthusiasm alone does not solve.
The healthcare leaders who will navigate 2026 most effectively are not those who move fastest. They are those who move with the clearest understanding of what they are buying, what they are committing their institutions to, and what their patients actually need from these tools.
That clarity begins with demanding more from the evidence, more from the vendors, and more from the governance frameworks that determine how these tools perform in the real world rather than on the benchmark leaderboard.
This content is part of the Computer Vision in Healthcare cluster. For related analysis, see our coverage of FDA 510(k) clearance data trends and statistical benchmarks, architectural frameworks for implementing Explainable AI in clinical environments, and the technical evolution from CNN to Vision Transformer models in diagnostic imaging.
Related Guides